Quick Note: What’s up with the new SARS-CoV-2 BA.2.75 and BA.5 variants?
You may have heard that there are a couple of new Omicron subvariants that are causing alarm: BA.2.75 and BA.5. Is this alarm just something for the media blogs to write about or do they pose some real threat? These subvariants have a few mutations that differ from Omicron, but we need to dive deeper to understand if these mutations mean much in terms of antibody evasion, pathogenicity, etc.
So, here’s a very short post on how these subvariants may affect us in terms of reinfection, needing a new booster, etc.
Receptor Binding Domain Mutations
BA.2.75 and BA.5 are very similar to the B.1.1.529 (Omicron) in the receptor binding domain (RBD) region.

Comparing to Omicron, the additional mutations I see in the RBD region are:
- D339H (only in BA.2.75, is originally G in the wild type)
- L371F (is originally S in the wild type)
- T376A
- D405N
- R408S
- S446G (only in BA.5, a reversion to the G wild type)
- L452R (only in BA.5)
- N460K (only in BA.2.75)
- F486V (only in BA.5)
- R493Q (a reversion to the Q wild type)
- S496G (a reversion to the G wild type)
Of these, there are are only a few that are at the S1 interface of the RBD, which is where some antibodies may bind in the “up” position.
Docking with an old Antibody
Some of the biggest questions we should be asking ourselves (if we’re vaccinated or if we’ve had COVID before) is “Can I get reinfected?” and “If I get infected, how bad could the infection be?”
In my previous work, I used a variety of serum-derived antibodies and simulated the binding affinity between the Fab region of each antibody with the RBDs of Alpha, Beta, Delta, and Omicron.
Repeating this in silico experiment on a smaller scale, I generated the RBD structures of BA.2.75 and BA.5 using AlphaFold2 and docked them (using HADDOCK 2.4) to an antibody called CC12.1.
CC12.1 was previously isolated from a SARS-CoV-2–infected patient and was shown to be specific for the RBD [PMID 32540903]. However, the neutralization ability of CC12.1 was measured using a much older strain of the virus. Perhaps we can use this as a proxy to understand how our vaccine-based antibodies, which are also from an early strain of SARS-CoV-2, may perform with these new subvariants?
BA.2.75

BA.5

Comparison
As you can see in the images above, the binding angle of the CC12.1 Fab is slightly different, but the overall binding is quite similar between the two.
At the interface between where the CC12.1 antibody would bind, there is only one mutation that is different between BA.2.75 and BA.5: F486V.
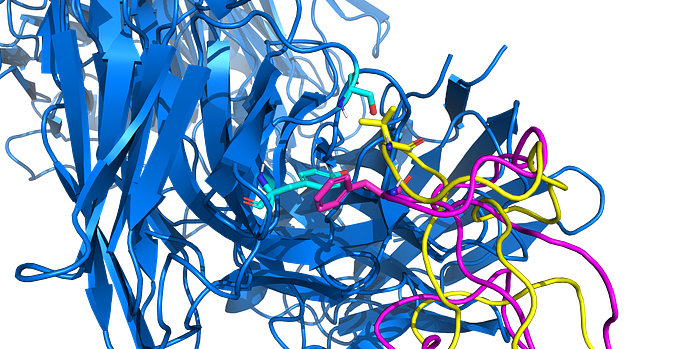
This change from a larger phenylalanine (aromatic) residue to a smaller valine residue may alter the CDR loop interaction/stabilization of the antibody. The replacement of an aromatic residue with another hydrophobic residue may reduce the ability for π-π interactions, but may alter the ability to form hydrogen bonds with other residues.
Also, if we see certain amino acid changes that favor non-aromatic residues, etc., we could use this information in future antibody/vaccine design. This being said, more in vitro analyses are needed to validate how these subvariants actually interact in the body.
Here are the HADDOCK predicted binding results:
Though this comparison is only using a single antibody, we do see ~30%-40% drop in overall binding affinity between BA.2.74 or BA.5 and the previous variants. However, this is a very similar decrease as we saw with the original Omicron variant (B.1.1.529). So, in terms of affinity, these new subvariants aren’t worse for this one (older) antibody.
Discussion
We are certainly seeing an increased need to update the existing vaccine (and booster) to match the current variant(s) that are circulating in the world today. If you’ve only had the vaccine, but haven’t been infected with Omicron (or another more recent variant), you may be at a higher risk. If you have been infected with Omicron recently, it’s not crazy to assume that the antibodies that resulted from that infection are likely to provide more protection against these new subvariants (as compared to the vaccine alone).
When we look at mutations that occur in any new subvariants, there are tons of things they can cause. From antibody evasion to increased binding to receptors in the body to nothing at all. We should really be careful as to not simply count the number of mutations, but to look a bit deeper as to what they may do (so as to not cause the media frenzy for no reason).
Resources
- BA.2.75 GISAID Accession: EPI_ISL_13302209.1
- BA.5 GISAID Accession: EPI_ISL_11017528
- GitHub Repo: https://github.com/colbyford/SARS-CoV-2_B.1.1.529_Spike-RBD_Predictions
Stay curious…
